
GLP‑1 Therapies May Spare Muscles With New Myostatin Blocker, While Retatrutide Use Stirs Controversy
Myostatin Blocker Shows Promise Against GLP‑1 Muscle Wasting
A new drug called apitegromab is being tested to counteract muscle loss linked to GLP‑1 weight‑loss medicines. The phase‑2 study, led by researchers at several U. S. academic centers, began enrolling patients in early 2025 and reports its first results this month. At the same time, clinicians are prescribing the experimental GLP‑1 agonist retatrutide without regulatory approval, prompting debate over safety and ethics. The conversation also includes a shift toward higher‑protein diets for patients on GLP‑1 therapy.
Health news
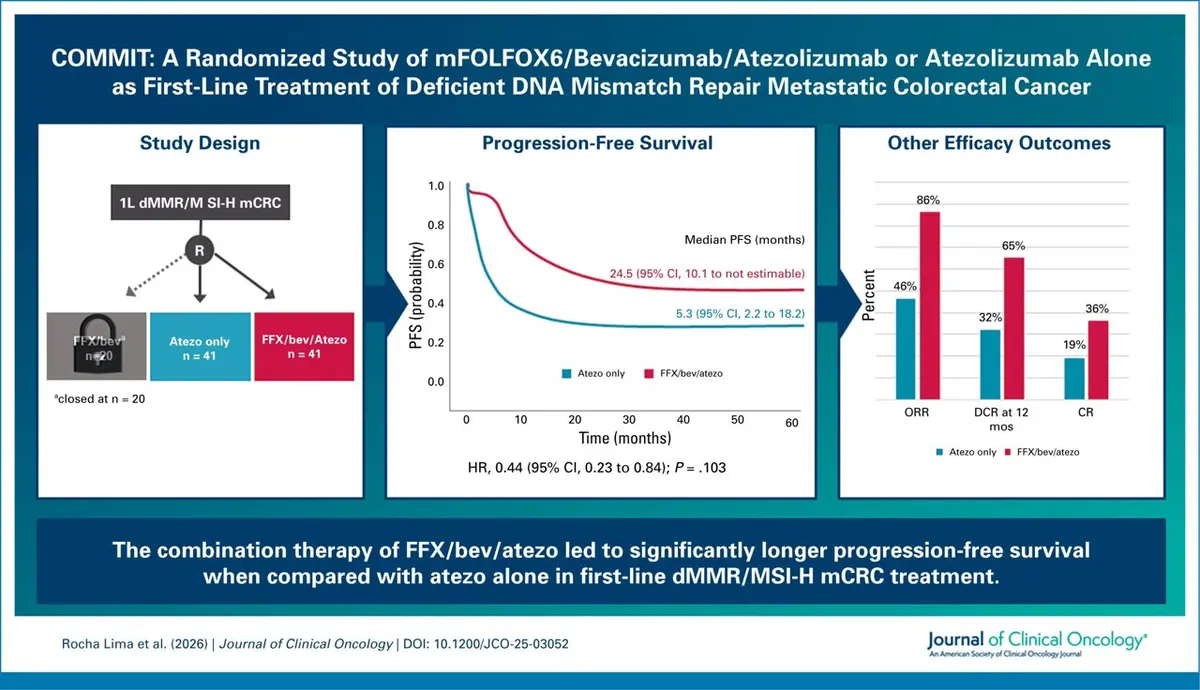 New Treatment Extends Life for Colorectal Cancer Patients
New Treatment Extends Life for Colorectal Cancer Patients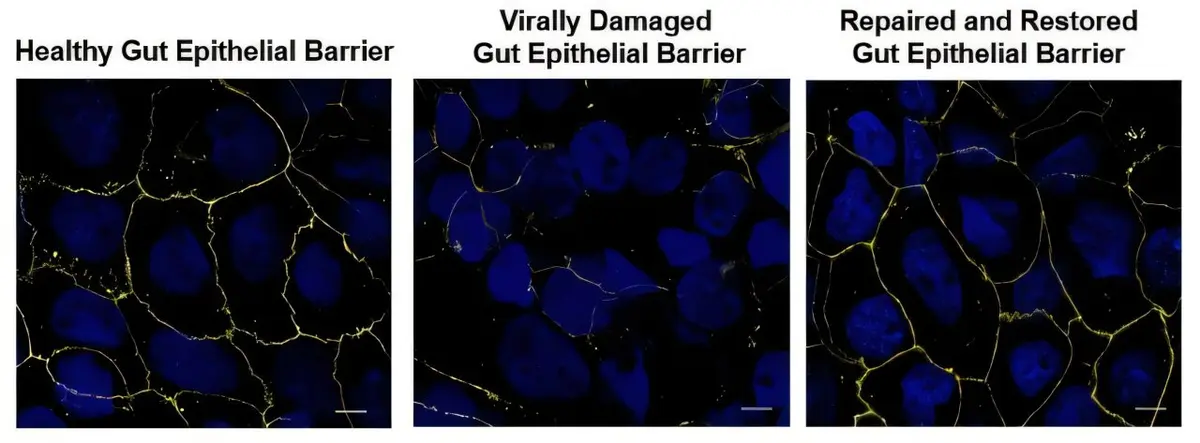 Probiotic Compound Shows Promise in HIV Treatment
Probiotic Compound Shows Promise in HIV Treatment FDA Experts Scrutinize New Melanoma Therapy
FDA Experts Scrutinize New Melanoma Therapy Sleep Changes in Older Women Could Signal Health Decline
Sleep Changes in Older Women Could Signal Health DeclineApitegromab works by selectively inhibiting myostatin activation, a pathway that normally limits muscle growth. In the double‑blind trial, participants receiving the drug alongside a standard GLP‑1 agent maintained or increased lean body mass, while a placebo group lost an average of 2.3 kg of muscle over 24 weeks. Researchers attribute the benefit to restored protein synthesis and reduced catabolism, suggesting that myostatin blockade can offset the catabolic effects of potent appetite suppressants. The study also reported no serious adverse events related to the myostatin inhibitor, a key safety concern for long‑term use.
The trial enrolled 120 adults with obesity who had been on GLP‑1 therapy for at least three months. Participants were randomized to receive apitegromab injections every four weeks or a matching placebo. By week 12, magnetic resonance imaging showed a 5 % increase in thigh muscle cross‑sectional area in the treatment arm, compared with a 3 % decline in the control group. Dr. Elena Ramirez, the study’s lead investigator, said the findings „demonstrate a clear mechanistic link between myostatin inhibition and preservation of lean mass in this population.” She added that larger phase‑3 studies are needed to confirm durability of the effect and to assess functional outcomes such as strength and mobility.
Why Are Some Doctors Prescribing Retatrutide Off‑Label?
Retatrutide, a next‑generation GLP‑1 receptor agonist, has not yet received FDA approval, yet a growing number of endocrinologists are offering it to patients seeking more potent weight loss. Physicians cite early data from phase‑1 trials indicating up to 15 % body‑weight reduction, which they argue outweighs the risks of using an investigational product. Critics warn that off‑label use bypasses the rigorous safety monitoring required for approved drugs, and that the long‑term cardiovascular profile of retatrutide remains unknown. The American Association of Clinical Endocrinology has issued a statement urging clinicians to enroll patients in formal trials rather than prescribing the agent independently.
If apitegromab’s benefits are confirmed, the drug could become a companion therapy for the expanding GLP‑1 market, protecting muscle mass while patients achieve weight loss. Meanwhile, the retatrutide controversy highlights the tension between rapid innovation and regulatory oversight. Health systems may need to develop guidelines that balance patient access with safety, especially as more high‑potency agents emerge. Ongoing research on protein‑rich dietary strategies may also provide a non‑pharmacologic avenue to preserve lean tissue, offering clinicians multiple tools to address muscle loss.
Frequently Asked Questions
What is myostatin and why does blocking it help? Myostatin is a protein that limits muscle growth. Inhibiting its activation removes this brake, allowing muscle cells to synthesize more protein and grow larger.
Is apitegromab safe for long‑term use? Early trials report no serious adverse events, but larger studies are required to evaluate safety over years of treatment.
Can patients obtain retatrutide legally? Retatrutide is not yet FDA‑approved, so it can only be accessed through clinical trials or compassionate‑use programs, not via standard prescriptions.
Content written by Dr. Nathan Cole for wellness-bio-radar.com editorial team, AI-assisted.